Diet and Destiny
On
If you have spent time in the American South, you know that Southerners barbeque, fry or deep-fry almost anything that moves or grows. The eponymous Southern fried chicken is a staple on lunch and dinner menus. Breakfast, of course, involves bacon, preferably crispy and carcinogenic. Sugar is shovelled into most things that aren’t fried, and many that are.
It resembles the post-transitional Scottish cuisine which gave the world the deep-fried Mars bar, deep-fried pizza and for the morning-after connoisseur, deep-fried haggis. These delights (and copious cigarettes) made Glasgow the heart attack capital of the world (1). Had I not had the good luck to be born 45 miles to the east, I would probably not have made it this far (2).
It was not always thus.
Prior to the 17th century, when the more numerous English started causing trouble, Highlanders were known for their strength, health and endurance. This was due in no small measure to their diet, which was based on such foods as oats, herring and game. These foods provided omega 3 HUFA’s, phlorotannins, avenanthramides and 1-3, 1-4 beta glucans, guaranteeing immunity from chronic inflammation and dysbiosis.
Remnants of this still exist in the Orkneys, where healthy life expectancy at birth is a respectable 75.1 years for women, and 69.3 years for men (3). The lowland city of Glasgow went to the deep frier, ultra-processed foods, and the dugs. Health expectancy in Glaswegian women and men is 60.4 and 54.6 years respectively (3).
Scotland is behind me now. In the Summer of Love, the noblest prospect a Scotchman ever sees lured me from the Athens of the North to the Great Wen and from there I made my way, by degrees, to the American South.
Just before the scamdemic, friends took me to a NASCAR race at Talladega and thence to The Ark, a former bootlegger joint, for dinner. It was a nostalgic experience. I probably consumed a half pint of Crisco during the meal as the only item on the menu not deep-fried was the perfunctory salad.
One evening of deep-fried catfish, gator and hush puppies won’t do lasting harm but if eaten regularly, this diet will kill you before your time.
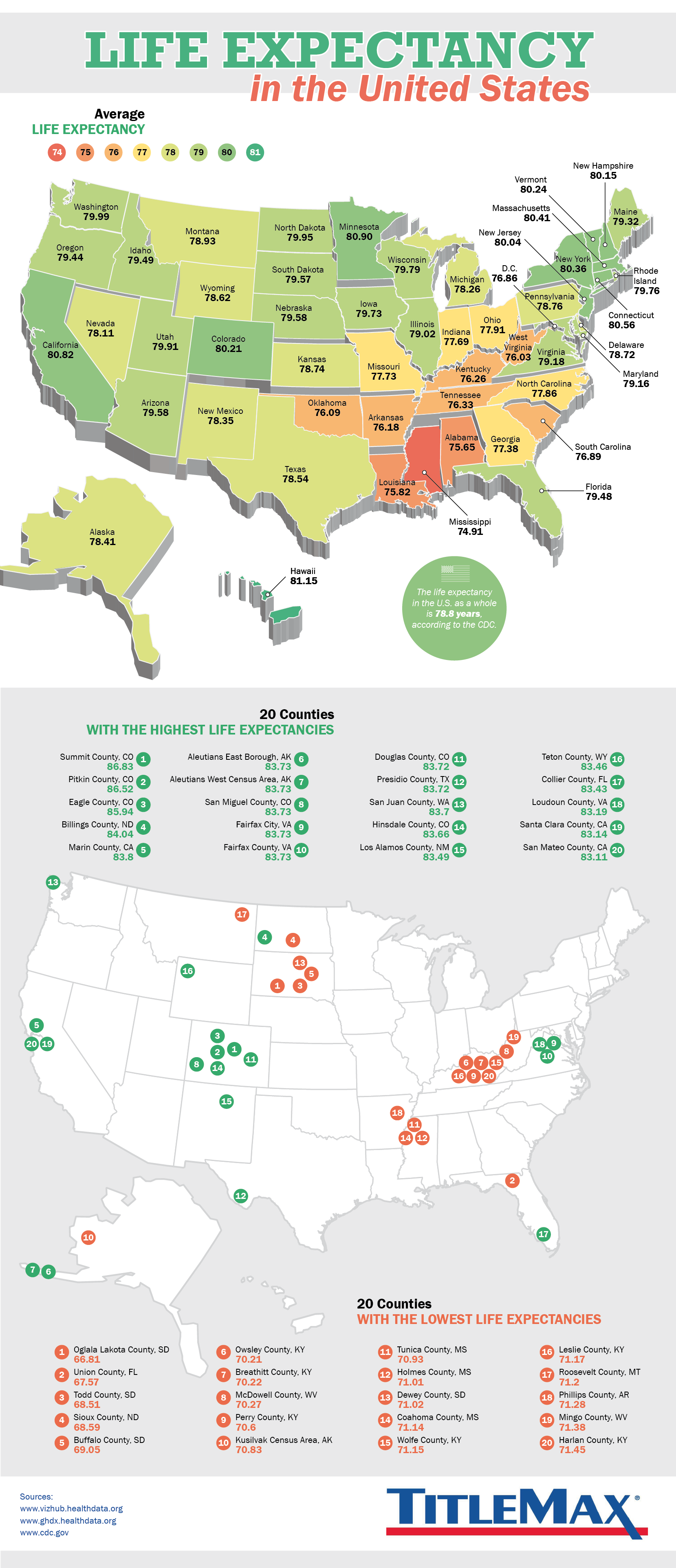
It’s no coincidence that Alabama, Arkansas, the Carolinas, Georgia, Kentucky, Louisiana, Mississippi and Tennessee are known, collectively, as the Stroke Belt (4). They could also legitimately be called the Obesity Belt (5), the Kidney Disease Belt (6), the Heart Attack Belt (7) or the Diabetes Belt (5); which means that they probably qualify for the NAFLD and GI Cancer Belts too. Unsurprisingly, they also hold the Lowest Life Expectancy Belt (8).
Too many Northerners look down their noses at Southerners, and accuse them of being racist, uneducated and in-bred. This is a sad reflection on Northerners who are not much different and certainly no better. It is just another form of stereotyping, identical to racism but invisible to those that practice it, that can be traced back to the imperial behaviour and attitudes of the Union.
The idea that Southern genes were to blame for their disability was disproved a quarter of a century ago by the Danish Twin study (9), when a team lead by the redoubtable James Vaupel edtablished that diet and lifestyle was responsible for 80% of health and life expectancy. It is the Southern diet and lifestyle which lie behind those straining Southern belts.
Climate is one factor. When temperatures and humidity rise, frying and deep-frying generate far less heat in the home than firing up an oven; while the barbecue can be set up on the porch or in the yard. In summer, heat and humidity discourage physical exertion.
Poverty is another. Southerners are disproportionately poor (10), and many inhabit so-called food deserts where fresh and healthy food is thin on the ground. Against the many things poor parents cannot afford, it is easier to scrape up a few dollars to treat themselves and the kids to a soda or fries. These might taste good but have zero nutritional value, and they are rich in non-satiating calories. This is a Glaswegian thing too.
Here are some of the reasons why poverty and obesity have run somewhat in parallel for the last half century (11-14), although the rising tide of ultra-processed foods is now tipping the scalesa across all social classes (13-15).
Human behavioural ecology (HBE) is involved as well. In nations where the ultra-processed tsunami has washed traditional dishes away, HBE predicts greater obesity among the poor due to ‘rules’ learned in our evolutionary past. We were hard-wired to feast in calorie-rich environments because hard times would surely come; poorer folk have more hard times, and immediate concerns that push worries about long-term health into the background (13, 16-18).
Add palatal acclimatisation, hyper-marketing and social normalisation.
Once you sell your soul to ultra-processed foods, it’s hard to go back (19–20). In the background, the unceasing marketing of Big Phood’s excreta runs like an oil slick through the media. The recent introduction of fat roll models (21, 22) tries to persuade us that obese is healthy, even as Covid nails the lie (23).
Returning to the Stroke Belt and the Southern diet, a newly published paper provides some insight into just how hazardous this lifestyle really is. A team of scientists from both sides of the Mason-Dixon Line followed 21 thousand subjects for 10 years, monitoring their diets and health outcomes (24).
Those who ate Southern foods most regularly had a 46% higher risk of sudden cardiac death (SCD) than those who ate the least Southern diet. Conversely, the highest level of traditional Mediterranean food intake was associated with a 25% lower risk of SCD than those who were furthest from the Med diet.
BLM personnel might be interested to learn that there is an ethnic dimension here. Higher adherence to the Southern diet emerged as the main reason why blacks are twice as likely to develop hypertension (24), and are more obese (25) and more likely to die of heart disease (26) than whites. If black lives really matter, dietary advice and assistance is an obvious place to start.
As the Alabama / Massachusetts team had previously published similar findings derived from the same cohort (27, 28) this latest paper was no surprise. Neither was their guarded language. Despite the consistency of their findings, they limited themselves to observing ‘trends toward an inverse association of the Mediterranean diet score and a positive association of adherence to the Southern dietary pattern with risk of SCD.’
The study relied on self-reporting, allowing potentially substantial bias to creep in; but if anything, this probably downplayed the results. Data from other studies show that even if you do eat a Mediterranean diet, adding Southern-style foods reduces its health benefits (ie 29). The Medi group in the Alabama / Boston paper may well have back-slid – people do, after all – and so the comparative benefits of a full-time Mediterranean diet may be even greater.
The methodology of the paper was more significantly undermined, in my view, by the fact that the researchers found an association between higher consumption of sugar and reduced sudden cardiac deaths in subjects who had coronary artery disease at baseline. While no explanation was offered, it probably reflects a methodological anomaly or simple chance.
To recap, the Southern diet is characterized by large amounts of sugar and added fats, red and processed meats and fried foods. The Mediterranean diet is more plant-based, centering on vegetables, fruits, legumes, whole grains, olive oil and fish. But there is more to diet than just these two dietary data points.
Blue zone studies show that when you move past the Mediterranean diet, the incidence of non-communicable degenerative disease falls even further (30–33).
And if the Mediterranean seems too far away, there are hacks. Simply reducing your consumption of processed meats (ham, sausage,bacon) and increasing your intakes of plant-based foods, will cut your risk of heart disease by roughly 75% (34, 35).
For those who lean South, and don’t want to change their diet at all, there are more hacks. I have seen enough cases of individuals due for a coronary artery stent or carotid angioplasty, who were spared surgery after utilizing a blend of fish oils and amphiphile polyphenols. I have spoken to surgeons who scanned their patients pre-op to determine where to cut, but found to their astonishment that all atheroma had gone.
These omega 3 / amphiphile polyphenol reports are broadly in line with the Zutphen (36-39) and other studies, which found that eating oily fish was protective against heart disease and stroke while lean fish and commercial fish oil were not (40–43).
It is also consistent with a new data set from the Framingham Offspring Cohort (44) in which people with a higher Omega-3 index showed a significantly decreased risk of cardiovascular disease and increased lifespan, compared to those with a lower omega-3 index. A low Omega-3 Index was as powerful in predicting early death as smoking, making this a very important risk factor indeed.
Supplements will not take the place of community and ikigai (a sense of purpose), which are also associated with better health and life expectancy. If you know what you are doing, however, you can construct your own blue zone. Even in the South. Even in Glasgow.
Next week: Sharks do get cancer. Fish, on the other hand, may save us.
An amended version of this post was published here: EC nutrition, Editorial 18.3 (2023)

REFERENCES
https://www.nrscotland.gov.uk/files//statistics/healthy-life-expectancy/17-19/healthy-life-expectancy-17-19-report.pdf



{kind=link}